Rapid advances in technology have brought improvements in prosthetic components. In particular, prosthetic knees and ankle/foot complexes have made substantial advancements with the incorporation of computer technology. For example, microprocessor knees are relatively new; the X2 knee from Ottobock (Minneapolis, Minnesota) represents one of the latest and most advanced units and has just been upgraded.
Until recently, there have been no similarly functioning ankle/foot components except for the Proprio Foot from Össur (Foothill Ranch, California), which also provides powered dorsiflexion.
Also, recently BiOM introduced the BiOM T2 foot and ankle system with the added technology of powered plantarflexion to further normalize amputee prosthetic gait. Active patients who have successfully used a microprocessor knee, such as the X2, have generally paired that technology with a variety of foot/ankle components, ranging from passive-elastic units to advanced-energy storing units.
To normalize gait and improve biomechanics even further in select above-knee amputees, experts in the field have suggested combining a microprocessor knee with a powered foot/ankle complex. One potential obstacle to this combination, however, concerns the possible conflict between the active components of the individual units, such as over- or underengagement of component sensors. This situation, theoretically, could compromise patient safety. BiOM, however, provides training to prosthetic providers to address possible component integration issues, including microprocessor conflict and methods to safely use the components together. Once the prosthetist received this training, the patient in this study was fitted with the T2 foot and the X2 knee with excellent results and no perceived disadvantages.
The patient was a 32-year-old man with a right transfemoral amputation due to trauma from a blast injury, which occurred during Marine service in Iraq. He also had a gunshot wound to his left leg, which resulted in severe injury, but this limb was salvaged and now has good residual function. Before the trauma, the patient was very athletic and involved in long-distance running and bicycling. Once he recovered from his acute injuries, the patient expressed a desire to return to his previous high level of activity and sport participation.
The patient’s prior prosthetic experience involved many types of knees, both mechanical and microprocessor. These included the Rheo Knee (Össur), the C-Leg (Ottobock), and the X2 ankle/foot. He experienced limitations in walking up and down hills and walking through snow, sand, and mud. He also felt that placement of his foot was “inaccurate” in situations such as walking between crowded tables in a restaurant or down an aisle of occupied seats in a movie theater. Carrying objects, such as a milk carton in a grocery store, was also problematic, because the object had to be carried exclusively on his sound side.The experiences of these limitations pushed him to look for other prosthetic options that would offer better performance in these situations. Ultimately, he received the T2 ankle/foot with the X2 microprocessor knee after using a different combination for 2 years. He felt substantial improvements in all the aforementioned limitations and has been using the X2 and T2 combination ever since. The prosthetist provided training in both instances. For distance running, the patient uses the Flex-Run (Össur) Foot.
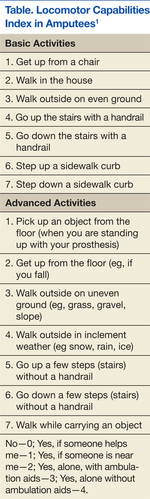
The Trinity Amputation and Prosthesis Experience Scale (TAPES) and the Locomotor Capabilities Index in Amputees (LCI) were used to assess his adjustment to the prosthetic and performance, respectively, before and after use of the aforementioned combination.
The LCI is a validated measure of lower-extremity amputees’ ability to perform activities with a prosthesis.1 The patient scored the maximum of 7 for all parameters of the LCI (a total of 28 parameters) while using his baseline prosthetic configuration of the X2 knee and the Triton foot (Ottobock). This score did not change when he used the X2/T2 combination (Figure 1; Table).
The TAPES Index is a validated measure of psychological adjustment to prosthetic integration.2 The measure consists of 12 items, rated 1 to 3 (1 = limited a lot; 2 = limited a little; and 3 = not limited at all). His total score was 25 using the X2 alone without the T2 but with the Triton foot. The patient reported that he was “limited a lot” on 2 activity measures (climbing several flights of stairs and running to catch a bus). This measure was reapplied after the patient used the T2 ankle/foot and X2 knee for several weeks. His new sum score was 36, the highest possible for this measure, indicating no functional, social, or athletic restrictions.
Furthermore, the patient reported other improvements, including an almost complete elimination of long-standing back pain, present since amputation. He reported he was able to climb hills with increased speed and less fatigue. The patient also reported he could stand more comfortably and don his shoes more easily, because the T2 would “bend.” Other subjective activity improvements included the ability to easily pick an object off the floor, step up curbs, walk on uneven ground, perform a mountain-climber exercise, and go through small spaces. He reported he was able to do all these activities previously, but the X2/T2 combination made these tasks easier than before to accomplish (Figures 2A and 2B).